






UPDATE: Karen Read is facing charges in the death of her police officer boyfriend, John O'Keefe. Opening statements are expected April 29. More
The Latest News
View All

The Court of Appeals ruled the judge at Weinstein's historic #MeToo trial prejudiced him and ordered a new trial. More

Podcast episode with testimony from Chad Daybell and Lori Vallow's inner circle: David Warick, one of the last people to see JJ Vallow alive. More

Christopher Gregor is charged with murder after he allegedly abused his six-year-old son and forced him to run on a treadmill. More

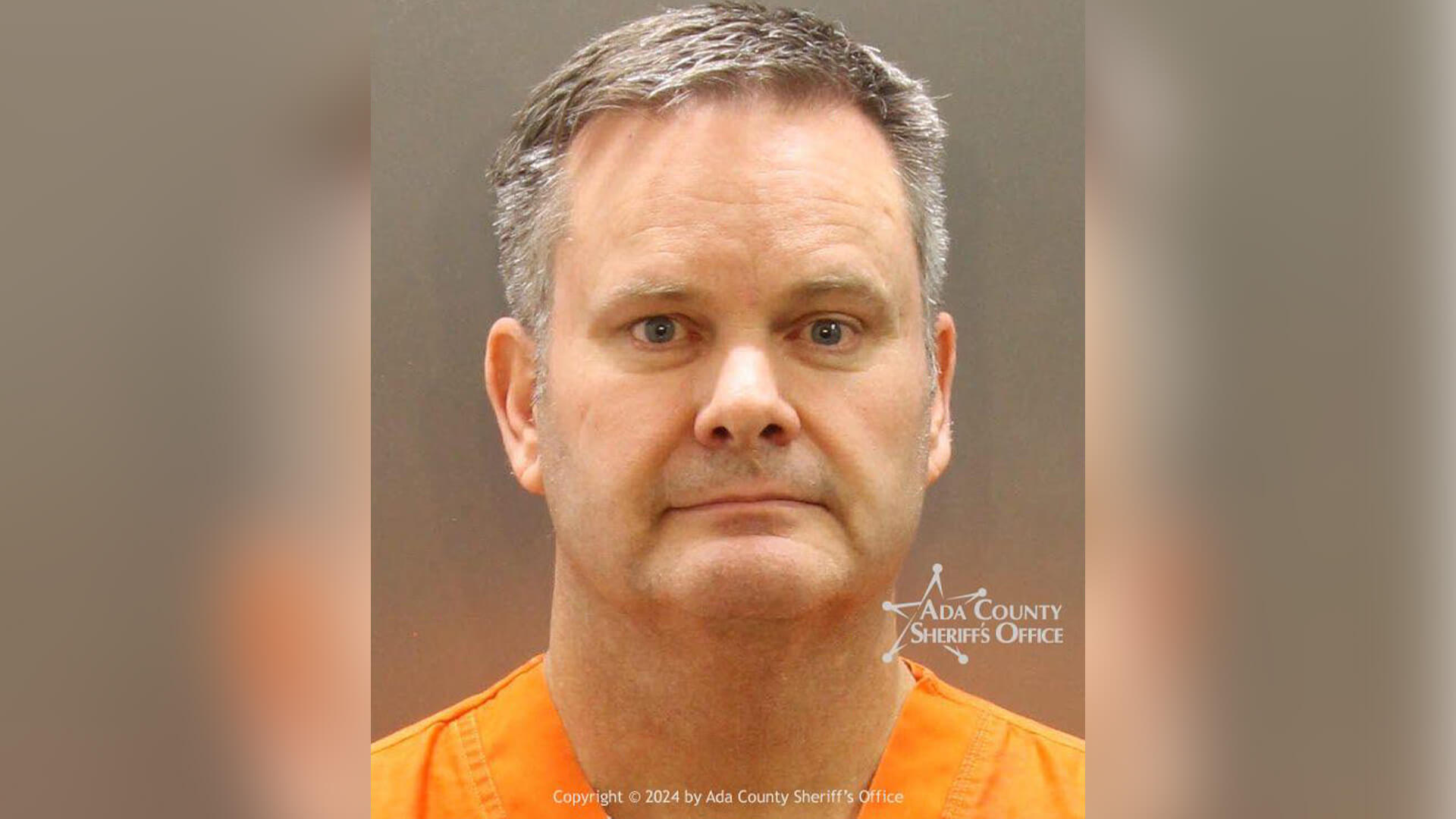
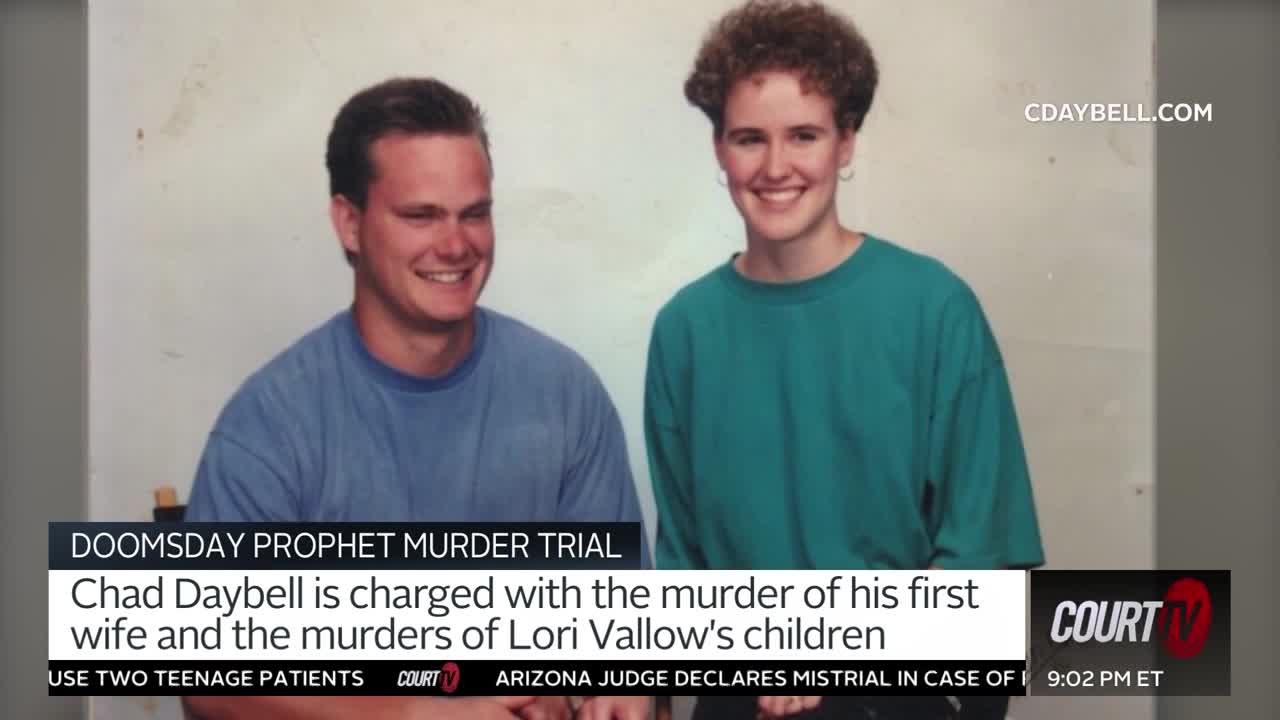
The trial of Chad Daybell, accused in the death of his first wife and the two youngest children of his second wife, Lori Vallow, is... More

Oklahoma prosecutors charged a fifth member of an anti-government group with killing and kidnapping Veronica Butler and Jilian Kelley. More

Investigators say Carly Gregg asked her friend whether she had ever seen a dead body before leading her to her mother, who had been shot. More

Stephan Sterns was charged with murder more than one month after he was charged with sex crimes after Madeline Soto's body was found. More
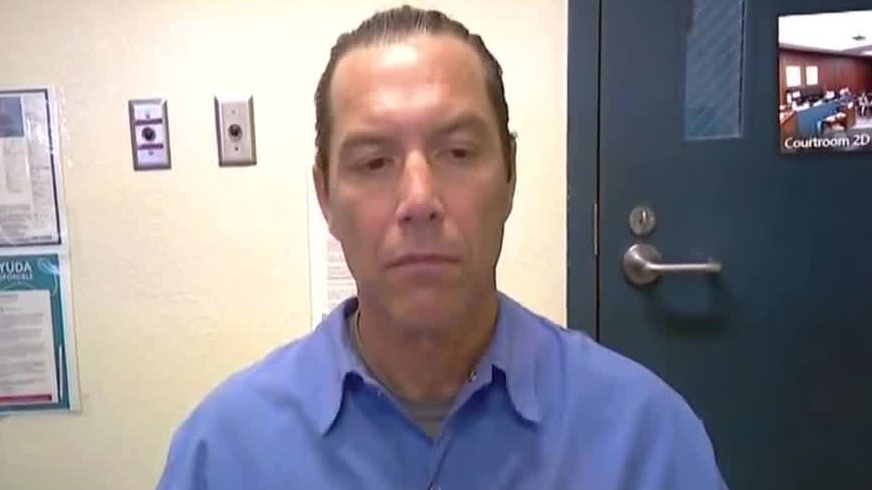
District attorney's office opposes motion filed by Scott Peterson's defense requesting DNA testing. LA Innocence Project now represents him. More

Kaitlyn Coones and Jonathon Jones, accused in the death of Jones' mother, were in court today for a hearing. More

The attorney representing Courtney Clenney on murder charges testified at a hearing regarding accessing the victim's laptop. More
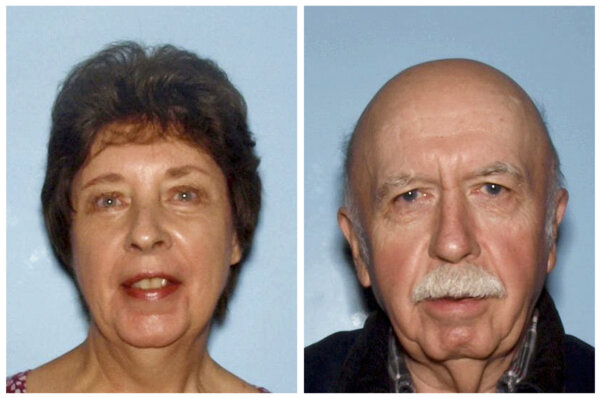
Ronnie "Jay" Towns is awaiting trial in the death of Bud and June Runion, who were found fatally shot in 2015 after allegedly responding to... More


TRIAL ARCHIVES


WI v. DAHMER (1992)
Jeffrey Dahmer is facing life in prison or admittance to mental institution for the killings of 15 boys and men.
WATCH NOW
SC v. MURDAUGH (2023)
Alex Murdaugh is accused of killing his youngest son, Paul, and wife, Maggie.
WATCH NOW
CA v. MENENDEZ (1993)
Brothers Lyle and Erik Menendez are on trial for the shotgun murders of their parents, Jose and Kitty Menendez.
WATCH NOW
SC v. COLUCCI (2018)
Michael Colucci is on trial for the 2015 strangulation death of his wife, Sara Lynn Colucci.
WATCH NOW

OH v. GROVES (2020)
Daniel and Jessica Groves are facing life in prison for the death of their baby whose body was found in a well.
WATCH NOW
NJ v. MCGUIRE
Melanie McGuire is on trial for the murder of her husband, whose dismembered body was found stuffed in multiple suitcases.
WATCH NOW
FL v. ANTHONY (2011)
Casey Anthony is on trial for the 2008 murder of her 2-year-old daughter, Caylee.
WATCH NOW